Uncategorized
Hereditary cancers aren’t just a women’s problem. Jewish men need to take precautions too.
Bill Harris, a veteran Los Angeles photojournalist, didn’t think much of it when one morning in 2012 he woke up and found a tiny blood spot on the T-shirt he’d slept in. The next morning, he found blood in the same place on his chest — and went straight to his computer.
“Online, I could find only three things that would cause a man’s nipple to discharge blood: being an avid runner, which I wasn’t; having a subtropical fungus, which I didn’t; and breast cancer,” he said. “That was a pretty big shock.”
Harris, then just a few weeks shy of his 61st birthday, immediately called his doctor, who ordered a mammogram and ultrasound. They confirmed a cancerous growth in his right breast. Ten days later, a biopsy came back positive. The next month Harris got a right mastectomy, followed by the removal of his left breast half a year later.
“I walked into a woman’s imaging center and had to get into a pink paper robe,” he recalled. “All the women in the waiting room were staring at me.”
Like many other Ashkenazi men, Harris never had considered that he might have been born with a harmful mutation of the BRCA gene, which elevates the risk not only of breast cancer, but also of melanoma and prostate, ovarian and pancreatic cancer.
“Hundreds of other mutations in the BRCA gene are just as dangerous, but they’re not specific to Ashkenazim,” said Dr. Robert Sidlow, director of the Male BRCA Genetic Risk Program at New York’s Memorial Sloan Kettering Cancer Center. About 1 in 40 Ashkenazi Jews (those of Eastern European descent) carries the harmful mutation, compared to about 1 in 400 in the general population.
“The vast majority of patients I see are relatives of women who have breast or ovarian cancer and then get tested,” he said. Of BRCA mutation carriers, Sidlow added, “Most men are pretty happy to enroll in some kind of surveillance program once they get over the initial shock.”
Sidlow is on the Men’s Leadership Council at Sharsheret, the national Jewish nonprofit organization that educates the community about cancer risks and supports those with breast cancer and ovarian cancer.
Elana Silber, CEO of Sharsheret (Hebrew for “chain”), says it’s crucial that men with a family history of cancer undergo genetic counseling screening for BRCA and other hereditary cancer mutations.
Genetic testing is possible via a standard blood or saliva sample.
While Sharsheret is primarily considered a women’s organization, it has been using November — nicknamed Movember for its focus on men’s health — for an awareness campaign focused on Jewish men’s cancer risks.
“This is not only a women’s issue,” Silber said. “Family history is so important. When a man shares his family history with his doctor, he may not realize that he should mention that his mother had breast cancer or that his sister had ovarian cancer, as these are not generally ‘men’s diseases.’ They are not aware that these cancers could mean that they themselves are at increased risk for cancer and that they can pass on these mutations to the next generation – their daughters and their sons.”
If someone discovers he (or she) is a carrier of one of the genetic mutations with elevated cancer risks — not just BRCA but also such mutations as ATM, TP53, CHEK2, and PALB2 — there are various precautions they can take for themselves and their children. They can monitor their own health more closely, they can get encourage their children to test to see if they are carriers and, for any future children, take steps to prevent the mutated genes from being passed down.
For example, couples can conceive via in vitro fertilization, or IVF, and then test the embryos before implantation to ensure that only those unaffected by the genetic mutation are implanted.
While most women are aware of the risks of breast cancer, men generally are not — even though the disease strikes 2,500 men in the U.S. every year and kills about 500 of them, according to Sidlow. About 1-2% of men with the BRCA1 mutation and 6-7% of men with the BRCA2 mutation will develop cancer by age 80.
“This is why we recommend periodic mammograms starting at about age 50 for men who carry a BRCA2 mutation,” Sidlow said. “We like to educate these men on how to check their chests once a month and have a clinician do a breast checkup on them once a year.”
Since the BRCA1 and BRCA2 mutations also make prostate cancer more likely, men with either mutation should get PSA (prostate-specific antigen) levels in their blood tested annually beginning at age 40, rather than 50, the age at which screening generally begins, Sidlow said.
Sharsheret has been promoting the importance of learning one’s family history, genetic counseling and screening among both men and women. The 20-year-old organization also runs various peer support networks, offers financial assistance to cancer patients, provides mental health counseling and guidance to patients, caregivers, and their friends, and seeks to educate the broader Jewish community about cancer risks and support.
Peggy Cottrell, a certified genetic counselor at Sharsheret, said men in general are more reluctant to get regular checkups than women.
Ashkenazi Jewish men are at elevated risk not just of breast and prostate cancer but also of pancreatic cancer. Pancreatic cancer is particularly difficult because it’s tough to detect early enough and hard to treat. The five-year survival rate is only 11%. About 2% of BRCA1 carriers and 4% of BRCA2 carriers will develop pancreatic cancer, Sidlow estimated.
“Usually by the time pancreas cancer is clinically detected it has already spread microscopically to the liver,” Sidlow said. “But pancreas cancer is potentially curable if caught when the tumor is extremely small.”
Even among those with elevated risks, certain behaviors can improve one’s odds, such as avoiding obesity, smoking and excessive alcohol consumption.
Harris, the California photojournalist, is still fighting at age 71. While he overcame breast cancer 10 years ago, last year he was diagnosed with ampullary cancer, a rare disease related to his BRCA2 status that was discovered thanks to his participation in a UCLA study. Surgeons have removed his gall bladder, half his pancreas and part of his small intestine, and he has had to endure eight rounds of chemotherapy.
“I’m still working through the aftereffects of the chemo. I have to eat smaller quantities than before and take enzymes to supplement my digestive processes,” Harris said.
Meanwhile, his 37-year-old son discovered that he, too, carries the BRCA2 mutation, and he had a double prophylactic mastectomy and reconstruction at age 30 — just to be on the safe side.
“If there’s any history of breast, ovarian or prostate cancer in your family, get tested genetically so that you’re informed,” Harris advised. “Diagnoses happen way too late for men, and the danger is too big.”
—
The post Hereditary cancers aren’t just a women’s problem. Jewish men need to take precautions too. appeared first on Jewish Telegraphic Agency.
Uncategorized
How the Global Religious Landscape Changed from 2010 to 2020
Muslims grew fastest; Christians lagged behind global population increase
• Christians are the world’s largest religious group, at 28.8% of the global population. They are a majority everywhere except the Asia-Pacific and Middle East-North Africa regions. Sub-Saharan Africa has surpassed Europe in having the largest number of Christians. But Christians are shrinking as a share of the global population, as millions of Christians “switch” out of religion to become religiously unaffiliated.
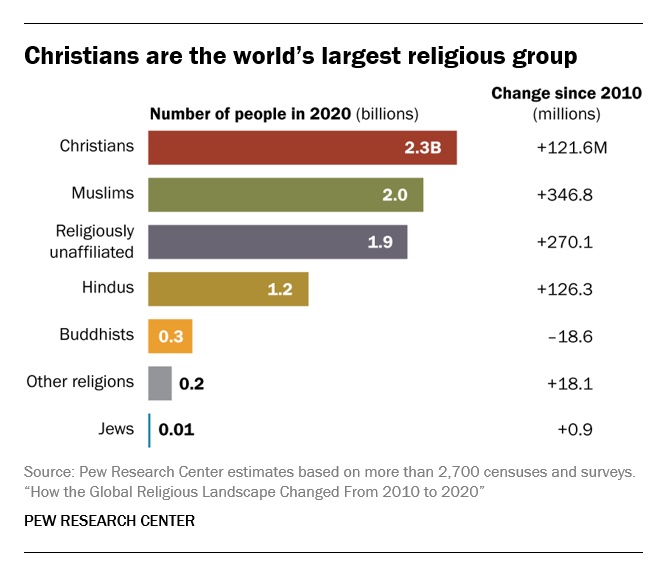
• Muslims are the world’s second-largest religious group (25.6% of the world’s population) and the fastest-growing major religion, largely due to Muslims’ relatively young age structure and high fertility rate. They make up the vast majority of the population in the Middle East-North Africa region. In all other regions, Muslims are a religious minority, including in the Asia-Pacific region (which is home to the greatest number of Muslims).
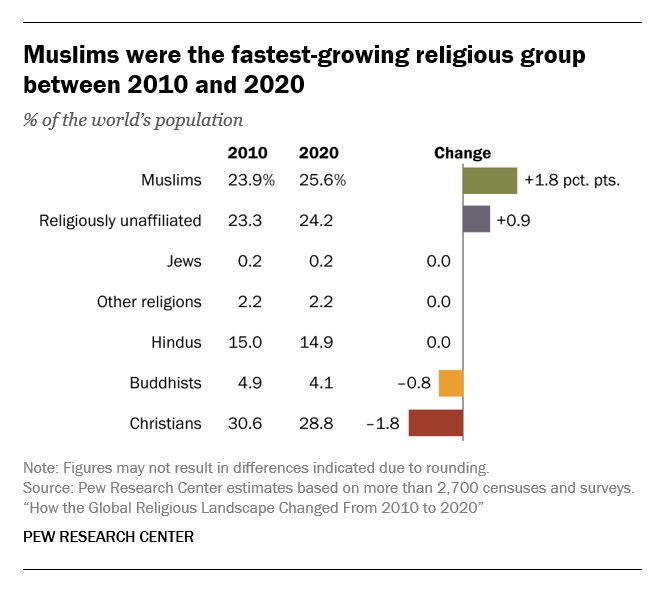
• The religiously unaffiliated population is the world’s third-largest religious category (24.2% of the global population), after Christians and Muslims. Between 2010 and 2020, religiously unaffiliated people grew more than any group except Muslims, despite their demographic disadvantages of an older age structure and relatively low fertility. The unaffiliated made up a majority of the population in 10 countries and territories in 2020, up from seven a decade earlier.
• Hindus are the fourth-largest religious category (14.9% of the world’s population), after Christians, Muslims and religiously unaffiliated people. Most (99%) live in the Asia-Pacific region; 95% of all Hindus live in India alone. Between 2010 and 2020, Hindus remained a stable share of the world’s population because their fertility resembles the global average, and surveys indicate that switching out of or into Hinduism is rare.
• Buddhists (4.1% of the world’s population) are the only group in this report whose number declined worldwide between 2010 and 2020. This was due both to religious disaffiliation among Buddhists in East Asia and to a relatively low birth rate among Buddhists, who tend to live in countries with older populations. Most of the world’s Buddhists (98%) reside in the Asia-Pacific region, the birthplace of Buddhism.
• Jews, the smallest religious group analyzed separately in this report (0.2% of the world’s population), lagged behind global population growth between 2010 and 2020 – despite having fertility rates on par with the global average – due to their older age structure. Most Jews live either in North America (primarily in the United States) or in the Middle East-North Africa region (almost exclusively in Israel).
These are among the key findings of a Pew Research Center analysis of more than 2,700 censuses and surveys, including census data releases that were delayed due to the coronavirus pandemic. This report is part of the Pew-Templeton Global Religious Futures project, which analyzes global religious change and its impact on societies around the world. Funding for the Global Religious Futures project comes from The Pew Charitable Trusts and the John Templeton Foundation.
Uncategorized
Antisemitism in some unlikely places in America
By HENRY SREBRNIK Antisemitism flourishes in a place where few might expect to confront it – medical schools and among doctors. It affects Jews, I think, more emotionally than Judeophobia in other fields.
Medicine has long been a Jewish profession with a history going back centuries. We all know the jokes about “my son – now also my daughter – the doctor.” Physicians take the Hippocratic Oath to heal the sick, regardless of their ethnicity or religion. When we are ill doctors often become the people who save us from debilitating illness and even death. So this is all the more shocking.
Yes, in earlier periods there were medical schools with quotas and hospitals who refused or limited the number of Jews they allowed to be affiliated with them. It’s why we built Jewish hospitals and practices. And of course, we all shudder at the history of Nazi doctors and euthanasia in Germany and in the concentration camps of Europe. But all this – so we thought – was a thing of a dark past. Yet now it has made a comeback, along with many other horrors we assume might never reappear.
Since the Hamas attack on Israel on October 7, 2023, there has been a resurgence of antisemitism, also noticeable in the world of healthcare. This is not just a Canadian issue. Two articles on the Jewish website Tablet, published Nov. 21, 2023, and May 18, 2025, spoke to this problem in American medicine as well, referencing a study by Ian Kingsbury and Jay P. Greene of Do No Harm, a health care advocacy group, based on data amassed by the organization Stop Antisemitism. They identified a wave of open Jew-hatred by medical professionals, medical schools, and professional associations, often driven by foreign-trained doctors importing the Jew-hatred of their native countries, suggesting “that a field entrusted with healing is becoming a licensed purveyor of hatred.”
Activists from Doctors Against Genocide, American Palestinian Women’s Association, and CODEPINK held a demonstration calling for an immediate cease-fire in Gaza at the Hart Senate Office Building in Washington, D.C., Nov. 16, 2023, almost as soon as the war began. A doctor in Tampa took to social media to post a Palestinian flag with the caption “about time!!!” The medical director of a cancer centre in Dearborn, Michigan, posted on social media: “What a beautiful morning. What a beautiful day.” Even in New York, a physician commented on Instagram that “Zionist settlers” got “a taste of their own medicine.” A Boston-based dentist was filmed ripping down posters of Israeli victims and a professor at the University of Pennsylvania Perelman School of Medicine did the same. Almost three-quarters of American medical associations felt the need to speak out on the war in Ukraine but almost three-quarters had nothing to say about the war in Israel.
Antisemitism in academic medical centres is fostering noxious environments which deprive Jewish healthcare professionals of their civil right to work in spaces free from discrimination and hate, according to a study by the Data & Analytics Department of StandWithUs, an international, non-partisan education organization that supports Israel and fights antisemitism.
“Academia today is increasingly cultivating an environment which is hostile to Jews, as well as members of other religious and ethnic groups,” StandWithUs director of data and analytics, and study co-author, Alexandra Fishman, said on May 5 in a press release. “Academic institutions should be upholding the integrity of scholarship, prioritizing civil discourse, rather than allowing bias or personal agendas to guide academic culture.”
The study, “Antisemitism in American Healthcare: The Role of Workplace Environment,” included survey data showing that 62.8 per cent of Jewish healthcare professionals employed by campus-based medical centres reported experiencing antisemitism, a far higher rate than those working in private practice and community hospitals. Fueling the rise in hate, it added, were repeated failures of DEI (diversity, equity, and inclusion) initiatives to educate workers about antisemitism, increasing, the report said, the likelihood of antisemitic activity.
“When administrators and colleagues understand what antisemitism looks like, it clearly correlates with less antisemitism in the workplace,” co-author and Yeshiva University professor Dr. Charles Auerbach reported. “Recognition is a powerful tool — institutions that foster awareness create safer, more inclusive environments for everyone.”
Last December, the Data & Analytics Department also published a study which found that nearly 40 per cent of Jewish American health-care professionals have encountered antisemitism in the workplace, either as witnesses or victims. The study included a survey of 645 Jewish health workers, a substantial number of whom said they were subject to “social and professional isolation.” The problem left more than one quarter of the survey cohort, 26.4 per cent, “feeling unsafe or threatened.”
The official journal of the Alliance for Academic Internal Medicine concurs. According to “The Moral Imperative of Countering Antisemitism in US Medicine – A Way Forward,” by Hedy S. Wald and Steven Roth, published in the October 2024 issue of the American Journal of Medicine, increased antisemitism in the United States has created a hostile learning and practice environment in medical settings. This includes instances of antisemitic behaviour and the use of antisemitic symbols at medical school commencements.
Examples of its impact upon medicine include medical students’ social media postings claiming that Jews wield disproportionate power, antisemitic slogans at the University of California, Los Angeles (UCLA) David Geffen School of Medicine, antisemitic graffiti at the University of California, San Francisco (UCSF) Cancer Centre, Jewish medical students’ exposure to demonization of Israel diatribes and rationalizing terrorism; and faculty, including a professor of medicine at UCSF, posting antisemitic tropes and derogatory comments about Jewish health care professionals. Jewish medical students’ fears of retribution, should they speak out, have been reported. “Our recent unpublished survey of Jewish physicians and trainees demonstrated a twofold increase from 40% to 88% for those who experienced antisemitism prior to vs after October 7,” they stated.
In some schools, Jewish faculty are speaking out. In February, the Jewish Faculty Resilience Group at UCLA accused the institution in an open letter of “ignoring” antisemitism at the School of Medicine, charging that its indifference to the matter “continues to encourage more antisemitism.” It added that discrimination at the medical school has caused demonstrable harm to Jewish students and faculty. Student clubs, it said, are denied recognition for arbitrary reasons; Jewish faculty whose ethnic backgrounds were previously unknown are purged from the payrolls upon being identified as Jews; and anyone who refuses to participate in anti-Zionist events is “intimidated” and pressured.
Given these findings, many American physicians are worried not only as Jewish doctors and professionals, but for Jewish patients who are more than ever concerned with whom they’re meeting. Can we really conceive of a future where you’re not sure if “the doctor will hate you now?”
Henry Srebrnik is a professor of political science at the University of Prince Edward Island.
Uncategorized
The 2025 Toronto Walk (and talk ) for Israel

By GERRY POSNER There are walks and then there are walks. The Toronto UJA Walk for Israel on May 25, 2025 was one of a kind, at least as far as Canada and Jews are concerned. The number of people present was estimated to be 56,000 people or 112,000 total shoes. (How they get to that number is bewildering to me, since there is no one counting). This was 6,000 more than last year. Whether it is true or not, take it from me, it was packed. The synagogues in Canada should be so fortunate to get those numbers in total on High Holidays. The picture here gives you a sense of the size of the crowd.

This was my first walk in Toronto for Israel and I was with my granddaughter, Samantha Pyzer (not to forget her two friends whom she managed to meet at the site, no small feat, even with iPhones as aids). The official proceedings began at 9:00 a.m. and the walk at 10:00 a.m. There was entertainment to begin with, also along the way, and at the finish as well. The finish line this year was the Prosserman Centre or the JCC as it often called. The walk itself was perhaps 4 kilometres – not very long, but the walking was slow, especially at the beginning. There were lots of strollers, even baby carriages, though I did not see any wheelchairs. All ages participated on this walk. I figured, based on what I could see on the faces of people all around me that, although I was not the oldest one on the walk, I bet I made the top 100 – more likely the top 20.
What was a highlight for me was the number of Winnipeggers I met, both past and present. Connecting with them seemed to be much like a fluke. No doubt, I missed la lot of them, but I saw, in no particular order (I could not recall the order if my life depended on it): Alta Sigesmund, (who was, a long time ago, my daughter Amira’s teacher), Marni Samphir, Karla Berbrayer and her husband Dr. Allan Kraut and family. Then, when Samantha and I made it to the end and sat down to eat, I struck up a conversation with a woman unknown to me and as we chatted, she confirmed her former Winnipeg status as a sister-in- law to David Devere, as in Betty Shwemer, the sister of Cecile Devere. I also chanced upon Terri Cherniack, only because I paused for a moment and she spotted me. As we closed in near the finish, I met ( hey were on their way back), Earl and Suzanne Golden and son Matthew, as well as Daniel Glazerman. That stop caused me to lose my granddaughter and her pals. Try finding them amid the noise and size of the crowd – but I pulled it off.

As I was in line to get food, I started chatting with a guy in the vicinity of my age. I dropped the Winnipeg link and the floodgates opened with “ Did I know Jack and Joanie Rusen?” So that was an interesting few minutes. And I was not too terribly surprised to come across some of my Pickleball family. All of these meetings, along with spotting some of my sister’s family and other cousins, were carried on with the sound of the shofar as we moved along the way. In short, this was a happening. Merchants selling a variety of products, many of them Israeli based, were in evidence and, of course, the day could not have ended without the laying of tefillin, aided by Chabad, who have perfected the procedure to take less than a minute. See the photo. Chabad had a willing audience.
Aside from the joy of sharing this experience with my granddaughter, the very presence of all these Jews gathered together for a common reason made this day very special to me. However, there was a downside to the day. The downside was that, as we began to walk back to our car there was no other way I could figure out how to return when the rains came and came. While we walked faster, we were impeded by pouring rain and puddles. But Samantha wanted to persevere, as did I. We made it, but were drenched. My runners are still drying out as I write this two days later.
What with being surrounded by 56,000 people, the noise, the slow walking, and the rain, I can still say the day was a real highlight for me – one of the better moments since our arrival in Toronto in 2012. As well as the photos we took along the way, I have the reminder of the day, courtesy of the UJA, as evidenced from the photo. It was not just the walk, but the talk that accompanied the walk that made it so worthwhile for me. I would do it again, minus the rain.