

Local News
“Narrow Bridge” offers wonderful lesson in understanding the struggles individuals go through in grappling with questions of identity – in an often quite humorous fashion
Review by BERNIE BELLAN
Is it possible to produce a play that tackles the tremendous pressure any individual deciding to undergo a gender transformation must feel in a way that is both fascinating, yet very amusing? Add to that pressure yet more pressure though when not only is that individual changing their gender, they’re also becoming increasingly drawn to an orthodox form of their religion.
Such is the storyline of Winnipeg Jewish Theatre’s newest production, “Narrow Bridge,” written by Winnipeg playwright Daniel Thau-Eleff – on now at the Berney Theatre in the Asper Campus until March 19.
Although I was somewhat familiar with the background to this particular play (having followed its long development process and the many twists and turns it took until it was finally mounted this year), watching “Narrow Bridge” in a preview performance on Thursday, March 9, left me thinking that the work that had gone into honing “Narrow Bridge” from simply an idea for a story that began 10 years ago into a play that is at once riveting, amusing, and highly educational has been well worth it.
The play opens with the protagonist, played by Elio Zarillo, who is identified as “Sholem” in the playbill, explaining to the audience that – at this point in their life, they are a woman whose name is “Samantha” (or “Shoshana” in Hebrew). (And, despite the antagonism exhibited by so many conservatives to the use of “they” as a pronoun in place of “he” or “she”, while watching this play it is totally apparent why a non-specific pronoun is perfectly appropriate for non-binary individuals. Still, don’t be mistaken into thinking “Narrow Bridge” is some sort of didactic lesson in gender politics. Far from it.)
Samantha is soon joined on stage by sister Naomi, played by Alissa Watson, and mother Elaine, played by Rhea Ekler. Naomi announces that is she going to be married in six weeks to her boyfriend, Kevin, who is about to convert to Judaism. The dialogue in the opening scene is fast paced and often quite humorous.
Soon enough the action moves to a local Orthodox synagogue, where we are introduced to “Mendel,” played by WJT veteran Harry Nelken. If ever there was a perfect fit for a local actor to play an Orthodox Jewish scholar, Harry Nelken is it. Not only does he look every bit the part of an older Orthodox Jew, when he offers dissertations on the Talmud, which he does from time to time through the First Act, he is absolutely convincing as a scholar.
Moreover, as much as one might expect that expositions on certain parts of the Talmud might be somewhat dry – to say the least, Thau-Eleff clearly has a deep understanding both of the Talmud and Jewish history. There is a recurrent reference to the “Sanhedrin” (which, as is explained in the play, was the Jewish high court in the time of the Temple) in “Narrow Bridge”, and although I myself grew up learning about the Sanhedrin, having attended Jewish day school, Mendel’s explanation of how the Sanhedrin worked is quite illuminating.
Samantha’s increasing fascination with the Talmud, strange as it may seem in our modern-day world, is given great credibility by the back and forth dialogue between Samantha and Mendel. Samantha puts her quest for wanting to know more about Judaism in the form of one succinct question to Mendel, that sums up much of what this play is about: “What does it mean to be Jewish?”
Does it help though to have a familiarity with the Talmud and Jewish rituals, such as which occur during Shaabat on Friday evenings in observant Jewish homes, in order to fully understand what is going on in “Narrow Bridge?” I’m honestly not sure. I would rather expect, however, that any audience member who is interested in learning about what would motivate someone who is not Orthodox to begin with to want to become Orthodox, regardless of that audience member’s own background, would find much of what “Narrow Bridge” has to offer quite moving.
As the play develops, a good part of the First Act is taken up with Naomi’s upcoming wedding – and Samantha’s clear reluctance to play a major role in that wedding, notwithstanding Naomi’s request that Samantha be her maid of honor.
Again, there are plenty of clever exchanges between characters – with many pithy observations brought forward. At one point prior to the wedding, when tempers are running high, Naomi says to Samantha – in reaction to something their mother has just said: “There is one thing you have to understand about Jewish families. Everything is a matter of life and death!”
The First Act ends with the actual wedding. Suffice to say it’s not a Hallmark movie wedding.
As we learn more about Samantha’s transformation into Sholem in the Second Act, we also learn more about much of the negativity within the Orthodox Jewish community toward gay, bi, and transgendered Jewish individuals who would still like to remain observant. Thau-Eleff’s treatment of what is a highly contentious subject within the Orthodox world is done though with the utmost sensitivity. There is no condescension in how he depicts Mendel’s refusal to accept Sholem’s gender transformation.
Ultimately, Sholem does find his place within the observant Jewish community – largely thanks to the constant encouragement and support of his mother.
“Narrow Bridge” takes on some very tough subjects – with its recurrent theme being a search for identity – or identities, as the case may be.
Each of the actors handles their role with great sensitivity. Sure, there are many laughs, but there is also a great deal of heartbreak. No doubt a play like “Narrow Bridge” will resonate most deeply with a liberal audience – Jewish or non-Jewish, but it would have a clear meaning for anyone who has either struggled with finding their identity – or watched someone near and dear go though that struggle.
Local News
Nakba exhbit at CMHR – you can see it right here and make your own assessment

By BERNIE BELLAN (Posted June 26, updated July 19) The Nakba exhibit at the Canadian Exhibit for Human Rights opened to the public June 27. The morning before the exhibit was set to open to the public, (it had a private opening for invited guests the evening of June 26) we received a press release from the CMHR. That press release gave a very detailed description of what was in the exhibit, along with photos (supplied by Annie Kierans of the CMHR).
There is also a link right at the beginning of the press release that will allow you to watch the same videos that anyone attending the exhibit can watch. We reprinted what was sent to us without making one edit. We leave it to you to form your own opinion as to whether the exhibit is fair in its presentation, and whether it is lacking “context” – which is an accusation that has been levelled at the exhibit’s organizers by some representatives of Jewish organizations.
We have received many emails in reaction to the exhibit. If you have an opinion and would like to see it published on this website, you can send it to jewishp@mymts.net, but please indicate whether you would be willing to have it published on this website.
Here is what we received the morning of June 26:
Winnipeg, MB — June 26, 2026 — The Canadian Museum for Human Rights (CMHR) will open a new exhibit tomorrow that explores human rights violations related to the ongoing forced displacement of Palestinian Canadians.
Palestine Uprooted: Nakba Past and Present will be on display in the Rights Today gallery on Level 5 until 2028. Featuring personal stories told through artifacts and video testimonies, the exhibit presents Palestinian Canadians reflecting on their ongoing struggle for human rights. The small exhibit reveals enduring patterns of loss and resilience, helping visitors understand more about this contemporary human rights story.
Palestinian Canadian stories are now included alongside many other stories of forced displacement and human rights violations featured in the Museum’s galleries. Each of these stories contribute to our visitors understanding of human rights and help the Museum fulfill its mandate to foster reflection and dialogue.

Exhibition highlights
Personal stories and artifacts: Experience firsthand accounts from Palestinian Canadians sharing their journeys of displacement and memory through a series of five artifacts. Cases display artifacts like property deeds, house keys, and a traditional Palestinian embroidered dress, accompanied by short videos that deepen understanding of the impacts of displacement.
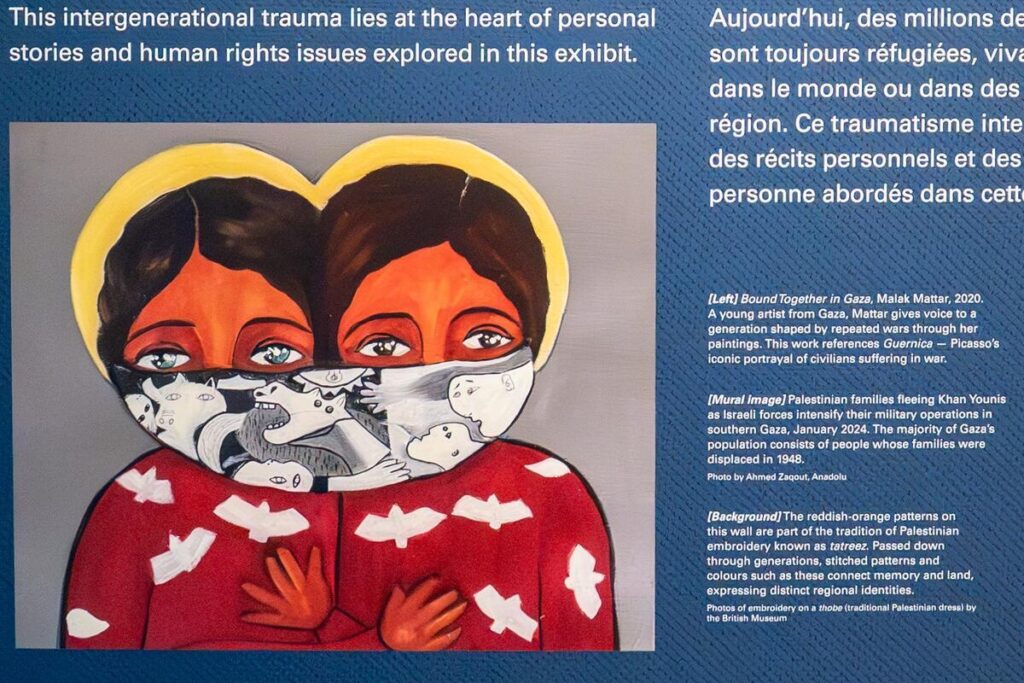
Powerful artworks: In her painting Bound Together in Gaza, Malak Mattar, a Gazan artist, captures the struggles and resilience of her generation shaped by conflict. Her work pays homage to Guernica, Picasso’s powerful masterpiece depicting civilian suffering during war.

Curfews and Closures, by Rajie Cook, bears witness to life under military occupation during the 2000–2005 Palestinian uprising, when curfews and closures were expanded and further limited basic rights and freedoms.

Cultural heritage: Discover traditional Palestinian embroidery called tatreez. Tatreez motifs and colours are tied to place, family history and regional identity. Patterns are associated with particular towns, villages or areas of Palestine. In this way, tatreez is a form of storytelling: a way of preserving memory, sustaining identity and expressing resilience across displacement and exile.
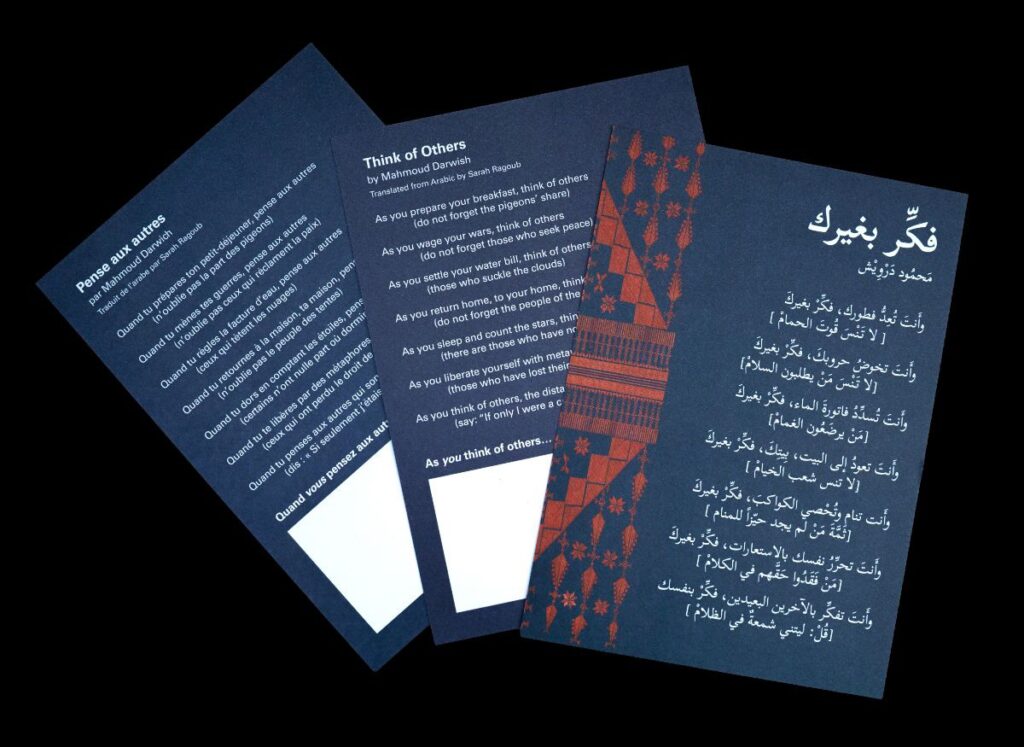
Poetry and reflection: Engage with Mahmoud Darwish’s evocative verses, inspiring personal reflection on exile, voice, and responsibility. Visitors can take a card containing Darwish’s poem and add a personal note, fostering ongoing dialogue beyond the exhibit.
Contemporary context: Witness striking images of current events in Gaza and the West Bank, connecting past displacement to ongoing struggles.
Quotes:
“No force can silence the truth we carry. Growing up in Canada, my children lived the Nakba through our stories. And now we watch it happen again, live, on our phones. When I see the images coming out of Gaza, I am not watching the news. I am watching my history repeat itself.” -Fouad Sahyoun, a Palestinian Canadian featured in the exhibit
“We developed this exhibit with a clear awareness that Palestinian Canadian voices have too often been marginalized, silenced or spoken over — and that anti-Palestinian racism affects whose stories are heard and whose suffering is recognized. That is why we intentionally centred Palestinian Canadian voices throughout the exhibit.” -Isabelle Masson, Curator of Palestine Uprooted
“Human rights matter precisely when they are inconvenient, when the question of who deserves the dignity of having their rights recognized is genuinely contested. These are the moments where having a national museum for human rights is most important.
There are people who believe this exhibit should not exist in its current form. There are people who believe it should have existed sooner. There are people who will visit this exhibit and feel that it does not say enough, and others who will feel it says too much.
We have listened to every one of these voices. We have reflected. And we have renewed our resolve to continue the difficult, sometimes contested, and often controversial work of building understanding about human rights. We are a museum grounded in Canada’s human rights framework, whose mandate requires us to bear witness to the full complexity of the human story. We are proud to open this exhibit because the story it tells will help achieve that mandate, and because this story belongs in the collective memory of Canadians.”
- – Isha Khan, CEO
Local News
A photo that’s being circulated on the internet about me

For those of you not familiar with nutjob Michael Kalo – the psycho who created the notorious “$hitler’s List” years ago and the same psycho who went after Ben Carr, well – now he’s obviously taken a strong disliking to the stance I’ve taken on the Nakba exhibit at the Canadian Museum for Human Rights. (You can read elsewhere on this website how I simply posted the entire exhibit as it is – and asked readers to form their own opinions.)
Kalo likes to send out emails to various individual using phony names – such as Frank Ostrowski. When people ask me (or asked Ben Carr) why we don’t take action against him, my answer is: What’s the use? He only basks in the attention.
So Michael – enjoy the attention you’re receiving. I know how much of an embarrassment you are to your wonderfully talented daughters.
Local News
Ami Hassan returning as owner of Falafel Place

By BERNIE BELLAN In a surprise move – and after more than a six-year absence as owner of Falafel Place (Corydon at Wilton) the legendary Ami Hassan has decided to return as owner of one of Winnipeg’s most famous eateries.
Long known for his sometimes irreverent attitude to his customers, e.g., “If you’re finished, get out!”, Ami decided to return to running Falafel Place after having retired years ago (or so he thought) from running the Corydon Avenue restaurant.
We asked Ami whether he’ll be sending a special invitation to Julia Roberts to come visit him at Falafel Place. He asked again: “Who’s Julia Roberts?” (Just kidding – he really does know how Julia Roberts is.) Read the story how Ami told her to leave the restaurant and come back later at Julia Roberts turned away from Falafel Place
Ami did note that when customers saw him inside the restaurant one recent day as he was getting it ready for the reopening Monday, August 10, over 20 of them came in asking him if he was open already.
We asked Ami whether the menu will be the same as it was when he last ran the place and he said everything will be the same.
Falafel Place will be open 7 days a week from 7 am – 2 pm. Remember, if you’re finished – get out!
