

Local News
Reaction to the valedictory address at the medical school convocation ceremony
Ed. note: We have received a number of inquiries, both from students in this year’s graduating U of M medical school class, and from former students (now practising physicians), asking whether we would print responses to what occurred during the convocation ceremony on May 16. In addition to their being published here, they will also be published in the June 5 issue of The Jewish Post.
We will continue to print whatever responses we receive as (and if) we receive them. In the meantime, here’ are the first two responses we received, on May 23:
May 23rd, 2024
Hello,
My name is Gregory Jackson. I am a member of the 2024 graduating class from the
Max Rady College of Medicine.
Our convocation has garnered more publicity than I would have ever thought. The
valedictorian’s address and subsequent aftermath compels me to act beyond my
traditional comfort zone.
A classmate of mine, Dr. Irvine, stated in an interview with the CBC that “from my
perspective, there wasn’t any students that were graduating that were upset with what was
being said”. I happened to be seated beside Dr. Irvine during convocation. Since Thursday, I
have been truly shocked, disheartened and embarrassed by what unfolded and its impacts
on our community. I regret not walking out during the valedictorian’s speech.
Boisterous cheers from emboldened supporters drown out the gasps and stunned
silence during the valedictorian’s address, turning a day that should have been shared joy
into a day of shared embarrassment. While I know that I cannot convince my classmates
on our disagreements in geopolitics, I am dismayed that our convocation was hijacked to
espouse reckless personal and aggressive political views.
I am writing this letter to show support and patience for the Dean, Dr. Nickerson, as
he navigates an appropriate and firm response. Furthermore, I am writing to formally
dissent and dispute the notion that the Class of 2024 is unified when sophistry
masquerades as advocacy. In the current climate of fear and violence, I respect those who
wish to remain anonymous to maintain their safety. Most importantly, I wish to vocalize my
support to my classmates, faculty members, and people living in our community who are
threatened and alienated by such rhetoric; I hope that our community can heal and that we
can re-aYirm an environment in which our Jewish members are safe, respected and loved.
Faithfully yours,
Gregory Jackson
Dr. Peter Nickerson, Dean and Vice-provost, Rady Faculty of Health Sciences
Michael Benarroch, President, University of Manitoba president@umanitoba.ca
Mr. Ernest Rady, 3420 Carmel Mountain Road, Suite 100, San Diego, California, 92121
CBC News, talkback@cbc.ca
Joe Hutchison at Dailymail.com
Roberta Lexier, Associate Professor, Mount Royal University rlexier@mtroyal.ca
Winnipeg Free Press
letters@freepress.mb.ca
I recall vividly that early morning September 1985 when I sat in my first class of Medical School at the University of Manitoba. The very first words spoken by the professor were ‘Primum non nocere’, which means ‘first do no harm’.
As physicians, we must use every means possible to gather an accurate history, using listening skills in a nonjudgmental fashion, and more often than not, creatively gathering collateral history from many sources. Dr. Gem Newman, to his credit, seems to be a passionate individual who cares about people. Unfortunately, the last few minutes of his speech made it clear that he cares only for some, on the basis of an incorrect history, leading to a disastrously incorrect diagnosis. He failed to take his own advice with respect to acknowledging one’s limitations rather than questioning if his opinion reflects fact. Nor does it seem that he consulted with those with more knowledge of the situation. His valedictorian address last week has caused harm: To the Jewish graduates, their families, as well as the Jewish community in the audience and abroad. To those who choose to believe the distortions of reality pertaining to the history of the region and current conflict. To those of us who know differently. To the truth.
Sadly, the response by the University and the media did not address specifically why Newman’s speech was so offensive. For that reason I feel compelled to provide the counter arguments, even if the damage has been done by the hundreds of thousands of views of his speech. After all, he’s a doctor. He should know what he’s talking about. Right?
Newman stated: “ I call on you to stand in solidarity with Indigenous people everywhere.” He either does not know or chooses to ignore the undeniable fact that the Jewish people are indigenous to that region of the Middle East for over 3700 years. He insinuated that the Jews are settler-colonizers, ethnically cleansing the Palestinians. Let me be perfectly clear. There have always been Jews living in that area since Abraham moved his family from Mesopotamia. Over the centuries the population had diminished due to invasions of the land resulting in massacres and exile. However, some always remained. Biblical reference, Jewish writings throughout the ages, numerous archaeological findings and even the Qu’ ran support the historical claim of the land of the ‘Israelites’, meaning the Jewish people. Never mind the fact that the term ‘Jew’ comes from ‘Judea’, just as ‘Arab’ from ‘Arabia’. His remark echoes the libelous accusation that the Jewish people are recent ‘colonizers’ who took over land belonging to others.
Prior to control by the British after WWI, the Ottoman Empire had conquered what is now Israel in the 1500’s. By the mid 1800’s the land was desolate and sparsely populated, as numerous published reports of the time have documented. I will provide two examples: In 1881, English cartographer Arthur Penrhyn Stanley wrote: “In Judea it is hardly an exaggeration to say that for miles and miles there was no appearance of life or habitation.” Mark Twain, in the mid 1800’s, wrote that one could walk from one end of Jerusalem to the other in an hour, At this time Jewish people and organizations started buying back the land from absentee Arab landlords at significantly inflated prices. By 1864, the majority population of Jerusalem, where our first and second temples were built dating back over 3,000 years, was Jewish. Following return of the Jews, with the economic, industrial and technological advances brought with them, Arabs began immigrating to the area as well. THAT is how the population increased; both Jews and Arabs began to repopulate the land. Again, written references from that era along with deeds to the land purchased by individuals and the JNF confirm this.
In 1948, the day after Sovereignty was granted to Israel, five Arab armies invaded Israel with the intent to exterminate all of the Jews and take over the new State. Arabs living there fled of their own volition or left by order of the Arab armies, with assurance that they could return to their homes after the Jews were gone. Lo and behold, Israel won the war against all odds. The 156,000 Arabs that remained became Israeli citizens, whose descendants are now 2 million, with equal rights as the Jews, Christians, Druze and every other citizen. Meanwhile 850,000 Jews were killed or forced to flee from many Arab countries across the Middle East, leaving their property and belongings behind.
Newman also claims that Israel is waging a genocidal war against Palestinians. The only genocidal attack was perpetrated by Hamas and associated Palestinian terror groups on October 7, 2023. I am not making a false claim. Ghazi Hamad in an interview October 23, 2023, as well as other Hamas leaders have been very clear about their intentions to ‘repeat October 7 again and again and again’. I have collected many interviews and videos from across the globe with calls to Islamist extremists to kill every Jew they encounter, as a religious duty. These calls for ‘Jihad’ and ‘Intifada’ coming from extremist Muslim religious leaders has now spread across the globe, and is even chanted by those who don’t know which River to Sea they want to clear the Jewish people from. Despite these threats of global annihilation of the Jewish people, Israel has sent out 7 million leaflets in Arabic with maps of safe zones, supplementing this with millions of phone calls, text messages and voice mails. The IDF ‘roof knocks’, which is sending a dud bomb as a warning to evacuate the area. Unfortunately, Hamas and UNRWA not only told civilians to ignore these warnings, they stole car keys and even shot civilians trying to leave for safe areas as reported by Palestinians and captured on voice recordings and video. No other military past or present goes to the lengths that Israel does to minimize civilian casualties.
This war is being fought in an unprecedented extremely complex war zone intentionally designed as such over the past 18 years. There are over 700 km of tunnels exclusively for Hamas’ use and protection. These terrorists fight in civilian clothes from hospitals, mosques, schools and civilian infrastructure, all of which lose protective immunity by law if used for such purposes. The referenced doctors, health care workers and journalists Newman insists Israel targets are not all altruistic innocents; many including hospital directors captured are longstanding members of Hamas. Rather than protecting their citizens, Hamas fight from beneath, beside and behind their men, women and children. The billions of dollars in aid funneled into Palestine over the years did not get spent on one single civilian bomb shelter. Despite this, Israel has still managed to achieve the lowest civilian:combatant death toll of ANY urban war hovering at about 1:1. This is even using the original Gaza MoH numbers prior to the exposure of manipulation of data at best, fabrication more likely, which led to the U.N. quietly backtracking and halving the number of women and children casualties. For seven months, those numbers had been broadcast to every news outlet and media source with impunity, and are still being quoted to this day. Not only are the numbers provided by Hamas grossly inflated, there are several analyses of the casualty data churned out by those terrorists that prove the patterns are statistically impossible.
You may also wish to verify the way the IDF conducts military operations with the Chair of Urban Warfare Studies of West Point, Major John W. Spencer.
Another resource is Colonel Richard Kemp of the British Army. Their opinions regarding whether a genocide is being waged on the Palestinians carry significantly more weight than Dr. Newman’s, I would think. The IDF is not called the ‘most moral army in the world’ for nothing.
On to the ‘famine” in Gaza. As of this writing, Israel has allowed entry of 427,981 tons of food, 59,930 tons of shelter equipment, 541 tanks of cooking gas, 23,260 tons of medical supplies, 34,940 tons of water. COGAT provides daily updates on humanitarian aid that has crossed into Gaza. Plenty of video evidence is available of Hamas confiscating the aid, shooting and killing civilians trying to get aid, and charging up to ten times the value of the aid (intended as donations, not to sell) which many cannot afford. There are estimates that Hamas has made close to $500,000 profit from this despicable abuse. The pier that the US provided has been targeted by Hamas rockets during and after construction. Videos are also posted daily of bustling markets full of produce in Gaza.
Apart from the poor taste the valedictorian displayed by using the last few minutes of his speech to grandstand, the greatest issue I have is that his claims do not contain fact. This is exactly the way the blood libels began, were spread, and continue to be spread. We witnessed the result of this less than a century ago and vowed ‘never again’. Yet here we are on our way to repeating history that apparently was not learned, with the help of people like Dr. Newman. We lost over 1/3 of the world Jewish population in the Holocaust, and 85 years later our census is still lower than it was in 1939; a mere 16 million, whose voice cannot come close to the volume of our adversaries.
I agree with free speech, but there must be accountability. There must be truth.
Annilea Gunn, MD, CCFP, FCFP
University of Manitoba Class of 1989
Local News
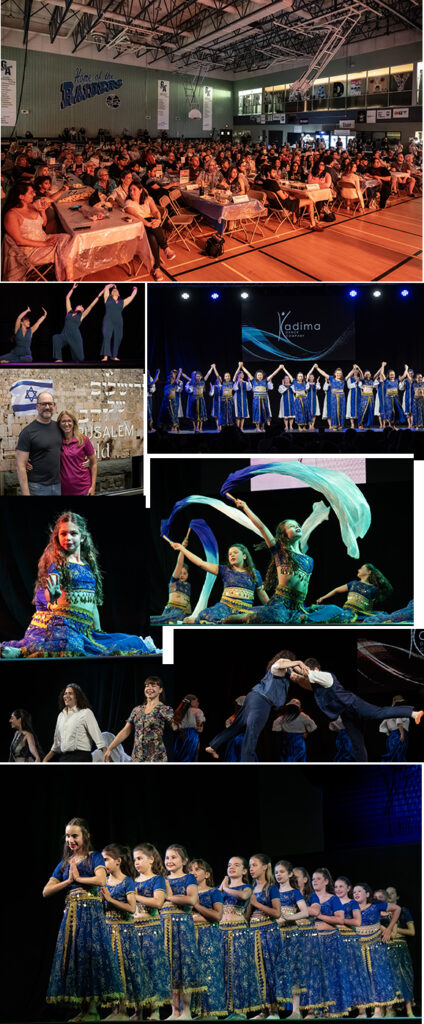
Scenes from Shalom Square 2026

Shalom Square – the Israel pavilion, is on until Saturday night, August 8. As usual, audiences have been packing the Rady JCC gym to watch entertainment provided by the Chai Folk Ensemble and Kadima Dance Troupe.
(All photos courtesy of Keith Levit)
Local News
Nakba exhbit at CMHR – you can see it right here and make your own assessment

By BERNIE BELLAN (Posted June 26, updated July 19) The Nakba exhibit at the Canadian Exhibit for Human Rights opened to the public June 27. The morning before the exhibit was set to open to the public, (it had a private opening for invited guests the evening of June 26) we received a press release from the CMHR. That press release gave a very detailed description of what was in the exhibit, along with photos (supplied by Annie Kierans of the CMHR).
There is also a link right at the beginning of the press release that will allow you to watch the same videos that anyone attending the exhibit can watch. We reprinted what was sent to us without making one edit. We leave it to you to form your own opinion as to whether the exhibit is fair in its presentation, and whether it is lacking “context” – which is an accusation that has been levelled at the exhibit’s organizers by some representatives of Jewish organizations.
We have received many emails in reaction to the exhibit. If you have an opinion and would like to see it published on this website, you can send it to jewishp@mymts.net, but please indicate whether you would be willing to have it published on this website.
Here is what we received the morning of June 26:
Winnipeg, MB — June 26, 2026 — The Canadian Museum for Human Rights (CMHR) will open a new exhibit tomorrow that explores human rights violations related to the ongoing forced displacement of Palestinian Canadians.
Palestine Uprooted: Nakba Past and Present will be on display in the Rights Today gallery on Level 5 until 2028. Featuring personal stories told through artifacts and video testimonies, the exhibit presents Palestinian Canadians reflecting on their ongoing struggle for human rights. The small exhibit reveals enduring patterns of loss and resilience, helping visitors understand more about this contemporary human rights story.
Palestinian Canadian stories are now included alongside many other stories of forced displacement and human rights violations featured in the Museum’s galleries. Each of these stories contribute to our visitors understanding of human rights and help the Museum fulfill its mandate to foster reflection and dialogue.

Exhibition highlights
Personal stories and artifacts: Experience firsthand accounts from Palestinian Canadians sharing their journeys of displacement and memory through a series of five artifacts. Cases display artifacts like property deeds, house keys, and a traditional Palestinian embroidered dress, accompanied by short videos that deepen understanding of the impacts of displacement.
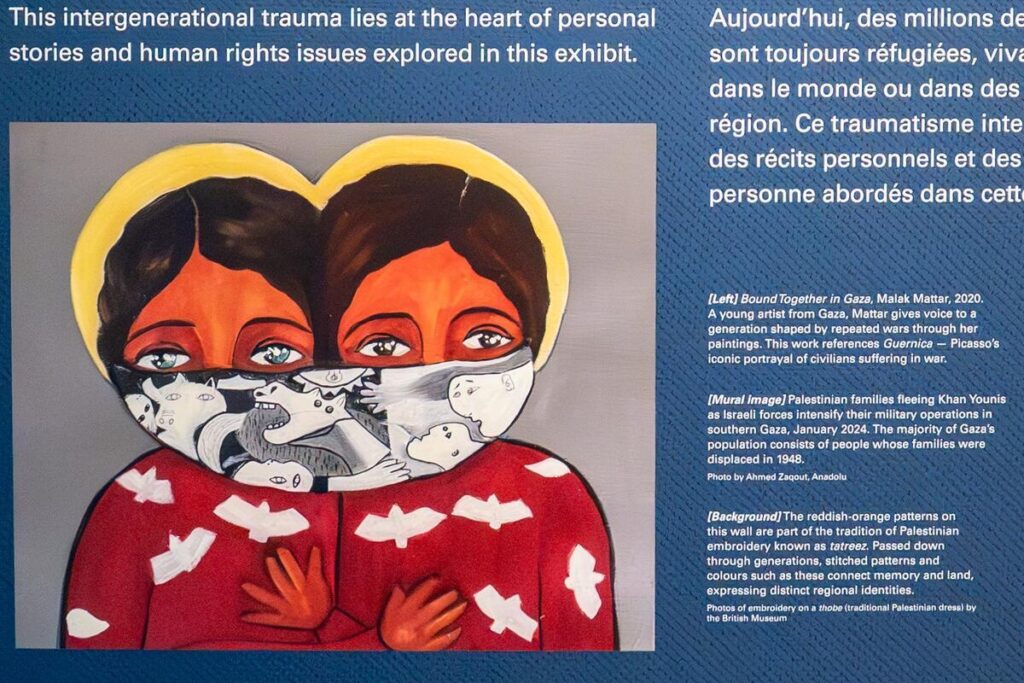
Powerful artworks: In her painting Bound Together in Gaza, Malak Mattar, a Gazan artist, captures the struggles and resilience of her generation shaped by conflict. Her work pays homage to Guernica, Picasso’s powerful masterpiece depicting civilian suffering during war.

Curfews and Closures, by Rajie Cook, bears witness to life under military occupation during the 2000–2005 Palestinian uprising, when curfews and closures were expanded and further limited basic rights and freedoms.

Cultural heritage: Discover traditional Palestinian embroidery called tatreez. Tatreez motifs and colours are tied to place, family history and regional identity. Patterns are associated with particular towns, villages or areas of Palestine. In this way, tatreez is a form of storytelling: a way of preserving memory, sustaining identity and expressing resilience across displacement and exile.
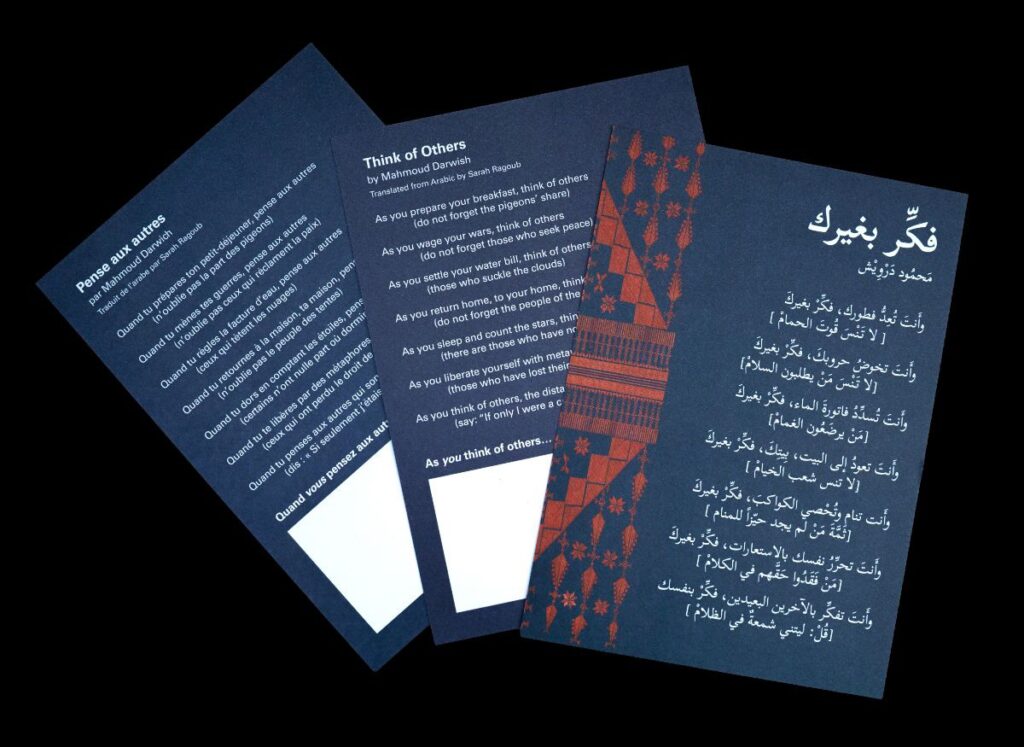
Poetry and reflection: Engage with Mahmoud Darwish’s evocative verses, inspiring personal reflection on exile, voice, and responsibility. Visitors can take a card containing Darwish’s poem and add a personal note, fostering ongoing dialogue beyond the exhibit.
Contemporary context: Witness striking images of current events in Gaza and the West Bank, connecting past displacement to ongoing struggles.
Quotes:
“No force can silence the truth we carry. Growing up in Canada, my children lived the Nakba through our stories. And now we watch it happen again, live, on our phones. When I see the images coming out of Gaza, I am not watching the news. I am watching my history repeat itself.” -Fouad Sahyoun, a Palestinian Canadian featured in the exhibit
“We developed this exhibit with a clear awareness that Palestinian Canadian voices have too often been marginalized, silenced or spoken over — and that anti-Palestinian racism affects whose stories are heard and whose suffering is recognized. That is why we intentionally centred Palestinian Canadian voices throughout the exhibit.” -Isabelle Masson, Curator of Palestine Uprooted
“Human rights matter precisely when they are inconvenient, when the question of who deserves the dignity of having their rights recognized is genuinely contested. These are the moments where having a national museum for human rights is most important.
There are people who believe this exhibit should not exist in its current form. There are people who believe it should have existed sooner. There are people who will visit this exhibit and feel that it does not say enough, and others who will feel it says too much.
We have listened to every one of these voices. We have reflected. And we have renewed our resolve to continue the difficult, sometimes contested, and often controversial work of building understanding about human rights. We are a museum grounded in Canada’s human rights framework, whose mandate requires us to bear witness to the full complexity of the human story. We are proud to open this exhibit because the story it tells will help achieve that mandate, and because this story belongs in the collective memory of Canadians.”
- – Isha Khan, CEO
Local News
Jewish Federation releases amounts to be allocated to each of its 12 beneficiary agencies
By BERNIE BELLAN I had been reporting on allocations given to the 12 beneficiary agencies of the Jewish Federation for over 11 years – until last year, when I took a break from covering our major Jewish organizations.
These past couple of months, however, I’ve gone back to looking at financial information for some of our major Jewish organizations, including the Jewish Foundation of Manitoba and Jewish Child and Family Services. (If you want to read my reports on the two Annual General Meetings held by those organizations you can find them elsewhere on this website.)
Over the years as well, I had also been adding to a table that I began to compile 12 years ago that showed comparison figures year over year for how much had been allocated by the Jewish Federation to each of its 12 beneficiary agencies. Even though I didn’t do any reporting on allocations by the Jewish Federation last year, I was able to obtain information about the 2025 allocations that I’ve reproduced in the table that you can see here. (That table only shows information for the past five years, although I do have tables showing information about allocations going back as far as 2014 that can be found on my website if anyone is interested.)
Looking at the figures for this coming year though, a couple of things stand out: For one, there will be no allocation for Aleph Bet Child Life Enrichment, just as there wasn’t one last year either. This comes after having received allocations for as long as I’ve been covering the allocations committee, so that might require some further investigation to find out why Aleph Bet Enrichment is no longer receiving an allocation. Secondly, there will be a small allocation for the Irma Penn School of Jewish Learning – as there was last year also, after a multi-year absence of the school applying for allocations. The Irma Penn School used to advertise in The Jewish Post & News when it was active, but I don’t recall seeing anything about it the past two years. At one time it was very popular among adults. It would be worth looking into how it functions these days. (Over to you, Myron. You used to write about the Irma Penn School.)
Also, the report of the Allocation Committee says: “The Jewish Learning Institute resumed their participation in the Allocations process after a hiatus of a few years to enhance their revitalized programming.” But the Jewish Learning Institute did receive funding in 2025 and 2024, so it’s not clear why the report says there was a “hiatus of a few years.” No big deal, really.
It’s always been interesting for me – and I’m sure for you, too, to look at trends: Which beneficiary agencies have been receiving the largest increases in allocations year over year or, as the case may be, the smallest increases in funding – relative to what other agencies received?
According to the report of the allocations committee, “The 2025-26 Combined Jewish Appeal Campaign raised $7,224,856 this year.”
That amount is $660,577 more than what was raised in the 2024-25 campaign, which was $6,864,279. While a portion of what was raised goes toward beneficiary agencies, another portion goes to Israel, another portion is to cover operating expenses of the Federation, and another portion goes to replenishing the Federation’s emergency fund, which was badly depleted during Covid.
Insofar as how much each of the beneficiary agencies receives,, each year the allocations committee of the Jewish Federation meets during the course of the year to decide how to allocates funds to the 12 beneficiary agencies of the Federation.
The allocations are to be given to the respective agencies on September 1.
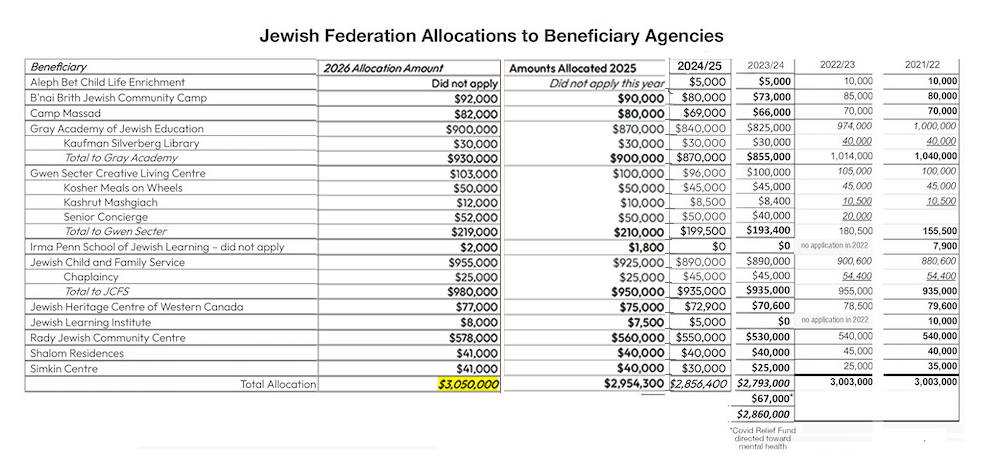
The total amount allocated to the Federation’s beneficiary agencies is $95,700 more than what was allocated last year, and $193,600 more than what was allocated in 2024. There will be a total of $3,050,000 allocated in 2026, compared to $2,954,300 in 2025, and $2,856,400 in 2024. Interestingly, the total amounts allocated in 2023 and 2022 were higher than what were allocated in 2024 and 2025, but the allocation to Gray Academy in 2022 was exceptionally high – $974,000, compared with $900,000 this year. In 2022 Gray Academy was still dealing with the fallout from Covid and the huge increases in costs that arose from having to resort to online teaching.
As well, until this year, the most ever allocated by the Jewish Federation to its beneficiary agencies was also in 2022 – when the community was still in the grip of the Covid crisis and total allocations were $3,003,000. At that time the Federation tapped into an emergency fund that it had on hand – and totally depleted that fund.
In its report the allocations committee went into some detail explaining its methodology and how certain criteria were given special attention when it came to determining allocations.
Each of the agencies had representatives appear before the committee. Those representatives were given 15-20 minutes to make presentations to the members of the committee and answer a series of questions pertaining to eight different criteria.
Here, in summary, are the main criteria the report cites as “priorities” when it came to deciding how much to allocate to agencies:
- Social isolation and lack of belonging: “Longing for belonging,” a desire for a
stronger sense of connection to the Jewish community and Jewish identification. - Seniors Isolation: Does this program address the problem of seniors’ isolation?
- Teen Program Continuity Gaps: Gaps in programming continuity limit teen
leadership opportunities. Peer connection programs across this demographic
must be prioritized. - Building Jewish Identity and Connection: Strengthening Jewish identification
ensures every program builds Jewish community through authentic Jewish content
and context. - Poverty and Financial Barriers to Participation: Financial challenges can prevent
community members’ full participation in Jewish life. - Accessibility and Inclusion for People with Disabilities: People with cognitive or
physical challenges face barriers to full participation in Jewish life. - Exclusionary or Unwelcoming Environments: Language and practices may
unintentionally exclude interfaith families, LGBTQ+ individuals, Jews of color, and
others. - Data on Participation and Community Needs: Do you have data available on who
participates in programs, who is underserved, and what impact programs have?
Even after having subjected each of the agencies to that sort of rigorous scrutiny, however, the fact remains that the sizes of the increases given to each agency were quite consistent with what had been given in previous years.
Here, for instance, are the increases that have been given to some of the agencies for the past three years:
Gray Academy – 2026 increase over 2025: $30,000; 2025 increase over 2024: $30,000
Gwen Secter – 2026 increase over 2025: $19,000; 2025 increase over 2024: $11,500
JCFS – 2026 increase over 2025: $30,000; 2025 increase over 2024: $25,000
Rady JCC – 2026 increase over 2025: $18,000; 2025 increase over 2024: $10,000
What it all boils down to, I would suggest, is that the allocations each of those agencies received are consistent with what they had received in previous years, notwithstanding the supposedly rigorous criteria that the allocations committee says it adopted in reviewing the presentations given by each agency.
