Local News
Lifesaving Israeli training coming to Winnipeg

By REBECA KUROPATWA
In 2016, when Magen David Adom (MDA) introduced the Life Guardian Program, thousands of Israelis with no medical training jumped at the opportunity to participate.
The Life Guardian Program added another layer of responders to emergencies to potentially save more lives with faster response time, by certifying or recertifying everyday Israeli citizens. Many participants had learned CPR as part of their army service or teacher certification, and others took first-aid basics for the first time.
When an emergency call is taken at the MDA dispatch centre, the computer system locates and contacts the closest Life Guardians and asks them to help save the life of a person in their close proximity, while also dispatching the closest medic or paramedic.
With an eye on the rise in anti-Semitic attacks in North America, Canadian Magen David Adom (CMDA) has come out with a training program that aims to give everyday people the know-how to help if they are in proximity to the site of a mass casualty incident.
The training is designed for anyone, no matter how much or how little medical training they possess, to give people the most basic tools to help save lives. It is called “The First 7 Minutes” and will soon be making its debut in Winnipeg.
The first training session is scheduled to take place on Feb 5th at 7 pm in the Rady JCC’s MPR (multipurpose room) and is being presented by CMDA and the Rady JCC. The special guest speaker will be MDA paramedic Don Sharpe, from Calgary who will train attendees and award certificates of training completion.
Sharpe has been a paramedic in Calgary for nearly 40 years. Four years ago, he had the fortune of training with MDA in Israel along with a group of other Canadian doctors.
“I’ve seen first-hand how an ambulance service should be run, and I think there are a lot of lessons there for us here in Canada – not just the actual frontline ambulance portion, but also for integration with hospital service, air service, and the Life Guardian Program,” said Sharpe.
“I tried several times to get that off the ground here, unsuccessfully, because, I think the community and cultural cohesion that seems to exist in Israel – we don’t have here.”
Sharpe grew up in the Jewish community of south west Calgary, though he is a Mormon by faith.
“As I grew older and started to watch what was happening with the rise of anti-Semitism and the violence against Jewish people and the State of Israel, I came to believe that Jews were precious,” said Sharpe.
“I wanted to work with a group that supported, not just the Jewish people, but also the State of Israel. So, when the opportunity came up…when I saw a presentation of a couple of doctors who had gone to Israel and worked with MDA, and they said they’d learned how to treat people on a moving ambulance…I was like, ‘Well, I can do that!’ They learned how to help people out in the field…and, I said, ‘I can do that!’”
Sharpe was especially impressed with MDA’s dispatch centre, which not only takes calls, but also provides lifesaving guidance over the phone until help arrives.
“We have so many people here now that, when an emergency occurs, they don’t know what to do,” said Sharpe. “The time I spent in MDA’s dispatch was really eye opening.
“When I first started in Canada, people would call 911 and we’d basically just take the call, start the ambulance, and hang up the phone.
“But, MDA’s idea that we can help people before the ambulance arrives is just brilliant. It makes such a huge difference.
“And now, to be able to teach groups of people, through “the First 7 Minutes” training, is perfect…groups of lay people on how to help a large number of people, casualties…in situations where everyone’s panicking. With just a little bit of training and some right thinking…there is now the idea that you aren’t powerless, that you can do something, you can cope. That little bit of training makes so much difference.”
Through “the First 7 Minutes” training, the first thing you will learn about is how to wrap your head around the possibility that you might be in a situation where 10 or 15 people are suddenly hurt and in need of help. The training will begin with a brief talk in order to best focus as much time as possible on practicing simulated mass casualty events.
“We start with something like a wall collapse, something without a bad guy, something that’s an accident rather than patients or blood,” said Sharpe. “This patient has a broken arm, this person’s unconscious, this person is bleeding from an abdominal wound…we go through determining who is in charge, how we know that person is in charge, where that person should stand and what s/he should do…what everyone else should do…and we also want to be alert for those people who are so freaked out by this that they don’t want to help at all.
“For those people, who might say they don’t like blood, I say, ‘Listen, there’s an important job for you. We need you to keep the people who aren’t hurt calm and look after them.’ I go, ‘Can you do that?’ And they say, ‘Oh yeah, I can do that.’”
The second simulated scenario might include an assailant. The third simulation will depend on the attendees and Sharpe’s observations on what should be further practiced.
“By the end of the training, you will walk away with some very basic understanding of how to work together as a team,” said Sharpe. “No matter who’s there, everybody can help a little bit. And, you know, if a situation ever truly arises where we have a large number of people hurt, you will remember the basics.
“You may not be good at it. Nobody ever gets good at it unless you spend the time I do treating patients, but you’ll be comfortable enough to say, ‘We can handle this and help people. We can take care of ourselves.’”
At the end, participants will receive a certificate. “I love the idea that people have to pay $10 for the training, because sometimes, when people just wander in and out and it’s free, they aren’t really paying attention,” said Sharpe. “Now that they paid, they’ll want to get their money’s worth, so they’ll have a real commitment to being there and learning this.
“I think communities need to learn to work together and to depend on themselves. And, it’s not only a good way to save lives in an emergency. It’s also a way to simply teach people to work together, so that, when they look at each other, they know they can depend on each other in an emergency. They’re well trained.”
CMDA and Sharpe are bringing the training to schools, synagogues, churches, and more.
While the topic is serious, you can expect Sharpe to include some humour along the way. “It can be a good time,” he said. “We have fun. People will walk away thinking, ‘I thought this was going to be pretty hard, but it was kind of fun.’”
Local News
Ami Hassan returning as owner of Falafel Place

By BERNIE BELLAN In a surprise move – and after more than a six-year absence as owner of Falafel Place (Corydon at Wilton) the legendary Ami Hassan has decided to return as owner of one of Winnipeg’s most famous eateries.
Long known for his sometimes irreverent attitude to his customers, e.g., “If you’re finished, get out!”, Ami decided to return to running Falafel Place after having retired years ago (or so he thought) from running the Corydon Avenue restaurant.
We asked Ami whether he’ll be sending a special invitation to Julia Roberts to come visit him at Falafel Place. He asked again: “Who’s Julia Roberts?” (Just kidding – he really does know how Julia Roberts is.) Read the story how Ami told her to leave the restaurant and come back later at Julia Roberts turned away from Falafel Place
Ami did note that when customers saw him inside the restaurant one recent day as he was getting it ready for the reopening Monday, August 10, over 20 of them came in asking him if he was open already.
We asked Ami whether the menu will be the same as it was when he last ran the place and he said everything will be the same.
Falafel Place will be open 7 days a week from 7 am – 2 pm. Remember, if you’re finished – get out!
Local News
The enormous – but little known role that Sheldon Berney played in the building of the Asper Campus

By BERNIE BELLAN Sheldon Berney passed away on July 28 in Palm Beach, Florida.
While his name may not be all that familiar to many members of Winnipeg’s Jewish community – other than the campus’s theatre having being named for him, at one time Sheldon Berney played an indispensable role in the building of the Asper Community Campus.
Six years ago I interviewed Bob Freedman about how the Asper Campus came about. Bob is one great story teller and if you want to see the entire interview (which is over an hour long, you can see it on YouTube at Freedman 2020 interview.)
The reason I’m harkening back to that interview now is to remind readers of the vital part that Sheldon Berney played in the building of the campus.
In fact, he was the the first president of the Asper Jewish Community Campus Board and, while the Berney Theatre is named for him and his picture adorns the entrance of the campus – along with Marjorie Blankstein’s and Bob Freedman’s, the contribution Sheldon Berney made to the building of the Asper Campus deserves to be recounted.
The story begins in 1986 when Bob Freedman had agreed to become the new executive director of what was then the Winnipeg Jewish Community Council. At the time he was executive director of Legal Aid Manitoba.
As Bob told me during our 2020 interview, “I said: ‘Look the only way I would consider doing that is if there was a commitment by the leadership of the WJCC to move the community forward.’ I had no intention of being a caretaker on a sinking ship.”
At the time, it should be noted, Winnipeg had begun to descend into the kinds of problems that have only been magnified in more recent years, including a deteriorating downtown – where the old YMHA was located, on Hargave – and to where an increasing number of parents were hesitant to send their children. Further, many young people had been leaving the city for better opportunities elsewhere.
Bob wanted to bring together a coalition of partners whose goal would be to develop a strategic plan that would move the Jewish community forward and revitalize it.
The first person he approached to be a part of that group was Marjorie Blankstein. As Bob explained, “I approached her and said ‘Marjorie, you’d be the perfect chair of our long-range planning committee’ and she agreed right on the spot. She didn’t need any convincing and that was May 2nd, 1986.
We then started the process, but we didn’t recruit Sheldon Berney, by the way, until a few years later,” he noted.
As Bob explained, together with Marjorie Blankstein, the two of them set out to assess community support for what had still not been identified as the campus project per se; it was more of a “sounding out” of as many different factions within the community as possible to determine how strong the determination was to move forward with a project that would complete rewrite the Jewish community’s direction.
I asked him during that interview how Sheldon Berney was eventually brought on board as a key member of the team.
Bob said that he didn’t really know Sheldon well, saying “I only met Sheldon once or twice. He was busy running the business. It was called “Reliance Products.'”
Here’s a brief excerpt from Sheldon Berney’s obituary as it appeared in the Globe & Mail that gives some detail about his business career, and his commitment to community service and philanthropy :
“Born to Ada (Loban) and Martin Berney, Sheldon lived an extraordinary life in Winnipeg before retiring to Florida. He built a distinguished career in business, joining his father at Reliance Products, which he expanded into an internationally respected manufacturer of plastic containers and camping equipment, celebrated for design excellence.
“A pillar of Winnipeg’s Jewish community and dedicated philanthropist, Sheldon chaired the Society of the Plastics Industry, the Manitoba Institute of Management, and the Young Presidents’ Organization. He served on the boards of the YMHA, CJA, and Victoria Hospital and was a core donor to the Canadian Museum for Human Rights. In the 1990s, he chaired the Asper Jewish Community Campus Board, taking immense pride in helping to bring the project to life.”
It was around the time that the idea for the campus project was being formulated that Sheldon Berney had sold Reliance Products, Bob Freedman recounted.
“Sheldon, at that time, was in his 50s and was basically retired,” Bob said.
“Even though he was not well known in the community,” Bob continued, “he had good relationships with people.” Sheldon Berney also socialized with Izzy Asper; they both had properties near each other in Florida, Bob noted.
“They shmoozed around and socialized…and we figured also he had credibility and had time on his hands, so we approached him, we briefed him, and convinced him we would need someone like him to do a job…In terms of how it was done it was a small nucleus of people who were really the movers and shakers on this….We started what was called the long-range planning committee” and Sheldon Berney “started recruiting people to serve on the committee – so we had financial people who were business people – who were ordinary people in the community.” (In fact, the name of the committee evolved to become the “Implementation Committee.”)
“I think we recruited Sheldon around 1989,” Bob recalled.
“There were two things he (Sheldon) said to us (Marjorie and Bob): “He said if I understand how things work with committees and boards – I have no patience for that…I don’t want to come to a ton of meetings. I want to have the authority to move forward and do things…and perhaps we have to spend money and need board approval – I understand that, but I don’t want the politics. I’ve got no patience for that.
“The other thing he said was when the time comes to raise money,” Sheldon said he wanted to check with certain people to see whether they would give their support to the project.
As Bob said (in his own inimitable way): “He didn’t want them to say you’re out of your f….king mind” and Sheldon would have wasted a year or two of his time.
“And Sheldon came back,” Bob said, “and every last one” of the people he had approached, which were about “four or five or six people and all of them said ‘go for it’ – and Sheldon Berney was on board, not only as a key fundraiser, but as someone who was very involved with finding the right location for the campus.
Bob told this somewhat amusing story about what happened when the initial proposal to build a community campus was for it be built at Waverley and Wilkes.
“But there were hydro towers there…and we had a public meeting and the screaming and the yelling that was going on…” and, as Bob explained, someone approached Sheldon and told him to hire someone with a Geiger counter (to measure radiation levels at the proposed site) – and this was already (19)93.” (It’s hard to imagine that the Asper Campus opened only four years later.)
Even though whoever measured the radiation levels at Waverley and Wilkes ultimately reported that there was more radiation “in your kitchen with appliances” than there was radiation from the hydro lines, Sheldon Berney was warned by someone else that “all we need god forbid is one kid in the school gets cancer and you will be dead in the water, so we agreed to move off” the Waverley and Wilkes site.
Once the plan to build at Waverley and Wilkes was dropped the focus turned to the possibility of buying what had been the Fort Osborne Barracks from the province.
Later on, when the fundraising was in full scale, Bob said that Sheldon Berney again played a key role in convincing Izzy Asper to scale back his insistence on having more representatives on the campus board than anyone else. Asper argued that if he puts up “$500,000 he should have 500,000 votes.”
According to Bob, it was Gerry Gray who told Izzy Asper that, in order for the campus project to be a true community project, if someone were to give “$1,000 that could be a really good gift considering their income and that gift is as important, if not more important than your five hundred thousand.”
But, Aper was persistent, Bob said, and one day Sheldon Berney phoned Bob and said Asper “is driving me nuts…so I said ‘Sheldon, I’ll tell you what. Why don’t you suggest to Izzy” that he contribute two million and “at that time two million was a lot of money…and tell him (Asper) he can have two people on the board.” (Bob explained that they were planning a nine-person board so having two representatives on the board would be a significant number, but at the same time the board was envisioned as not having much responsibility: It “would make sure carpets were cleaned, that the taxes were paid, and all that stuff.”
The next day, Bob said, Sheldon Berney met with Izzy and said to him: “Look, we got to put this to bed because I’m not sleeping at night.” Sheldon said to Izzy: “Here’s the deal: Two million bucks – you get two people on the board. He (Asper) says ‘okay.'”
But, as Bob noted, Izzy Asper continued to be very hands-on with the building of the campus and “he would drive Sheldon nuts and he would drive me nuts and he would drive all of us nuts.”
Sheldon Berney continued to play a key role in the campus project throughout its planning and construction. But when you realize that the campus actually went from an idea on paper in as late as 1994 to a fully finished project when it opened in 1997 (although construction continued even after the official opening in the summer of 1997), it’s rather amazing to contemplate how it all came together in such a relatively short period of time.
In an article in The Jewish Post & News published in May 1995 here is what my late brother Matt wrote about the groundbreaking ceremony for what was to become the Asper Campus. Berney, who was master of ceremonies at the ceremony was quoted as saying ” ‘Over the past six years, we’ve talked to people about the campus many times.’ “
The article continued: “The ceremony ended with Berney taking the controls of a huge yellow track excavator and scooping out a big chunk of earth.
“The groundbreaking was a ‘very exciting step’, he added, noting that demolition of some Fort Osborne Barracks buildings and campus construction would start the next week. ‘You’re all here to dream with me about the day in the summer of 1997 when we’ll all be back again to cut the ribbon on a campus that will be a source of pleasure for all of us.’ “
In the photo, Sheldon Berney (left), president, Asper Jewish Community Campus, is with Larry Hurtig, Winnipeg Jewish Community Council president, who is about to present Berney with a certificate of appreciation.
Later, in our September 17, 1997 issue, Matt chronicled the opening ceremonies of the Asper Campus, which were held on Sunday, September 7 of that year.
Again, Sheldon Berney was front and centre, as Matt noted in his report: “Sheldon Berney gazed at the crowd sitting in bridge chairs on the front lawn of the Asper Jewish Community Campus on the warm, sunny day.
” ‘Many times over the past several years, I’ve painted a mental picture of exactly this scene … ‘ the campus president told the crowd.
” ‘… Standing here at the formal dedication ceremony for the Asper Jewish Community Campus, feeling an enormous sense of pride, an enormous sense of accomplishment.’ “
And, because Sheldon Berney was a behind the scenes kind of guy we never really heard a lot of, yet he’s one of three people (the others being Marjorie Blankstein and Bob Freedman himself) to have plaques with their faces on them greeting anyone who walks through the front entrance of the campus we thought it appropriate to pay Sheldon Berney his proper due.
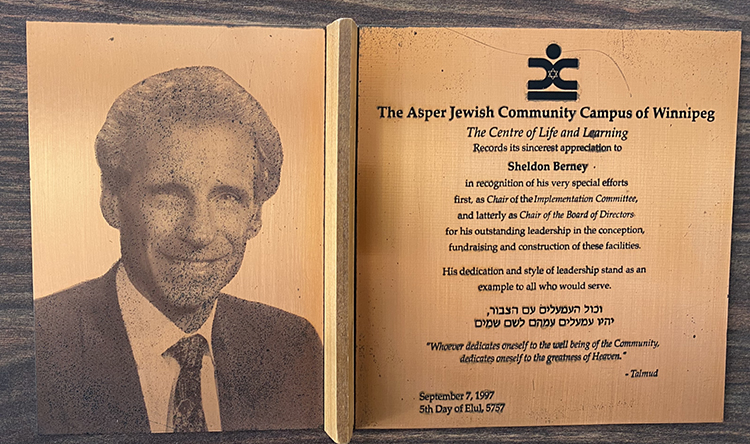
As the inscription on Sheldon Berney’s plaque notes:
The Asper Jewish Community Campus of Winnipeg
The Centre of Life and Learning
Records its sincerest appreciation to
Sheldon Berney
in recognition of his very special efforts
first, as Chair of the Implementation Committee,
and latterly as Chair of the Board of Directors,
for his outstanding leadership in the conception,
fundraising and construction of these facilities
His dedication and style of leadership stand as an
example to all who would serve.
Local News
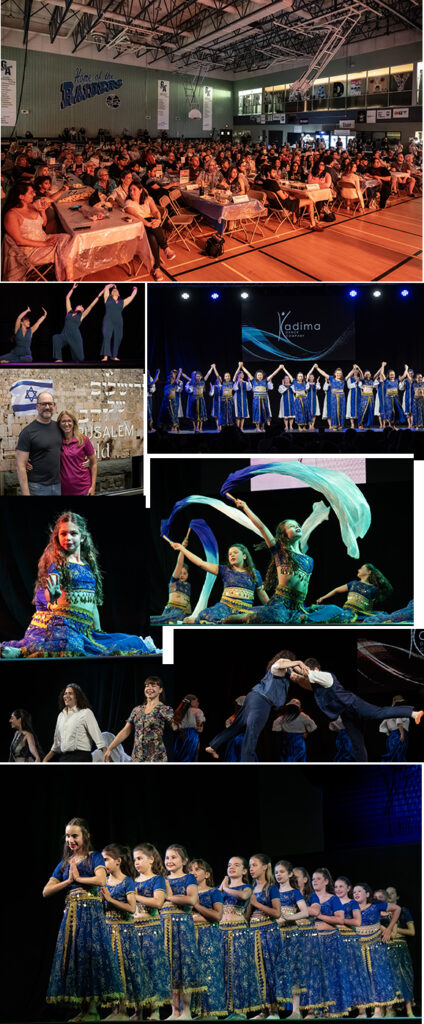
Scenes from Shalom Square 2026

Shalom Square – the Israel pavilion, is on until Saturday night, August 8. As usual, audiences have been packing the Rady JCC gym to watch entertainment provided by the Chai Folk Ensemble and Kadima Dance Troupe.
(All photos courtesy of Keith Levit)